
Histopathological Alterations in the Livers of Chronic Hepatitis Patients Exposed to Agent Orange/Dioxin in Vietnam

 , ,
, ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Areas and Subjects
2.2. Dioxin Measurements
2.3. Laboratory Tests
2.4. Histopathological Examination
2.5. Statistical Analysis
3. Results
3.1. Characteristics of the Subjects
3.2. Associations between TCDD and TEQ-PCDD/Fs Exposure and Laboratory Indices
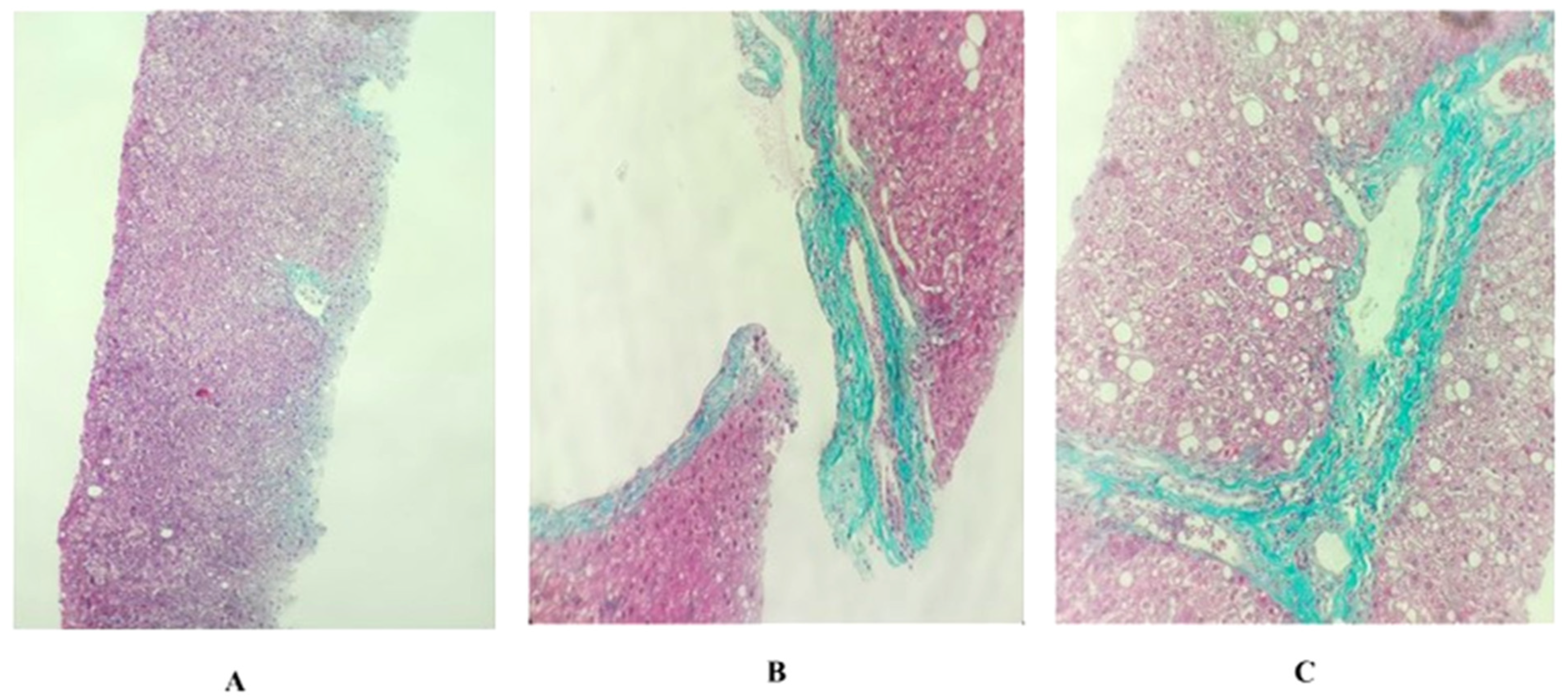
3.3. The Characteristics of Histopathological Damage
3.4. Associations between TCDD and TEQ-PCDD/Fs Exposure and METAVIR Scores
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Schecter, A.; Dai, L.C.; Thuy, L.T.; Quynh, H.T.; Minh, D.Q.; Cau, H.D.; Phiet, P.H.; Nguyen, N.T.; Constable, J.D.; Baughman, R. Agent Orange and the Vietnamese: The persistence of elevated dioxin levels in human tissues. Am. J. Public Health 1995, 85, 516–522. [Google Scholar] [CrossRef] [Green Version]
- Pocchiari, F.; Silano, V.; Zampieri, A. Human health effects from accidental release of tetrachlorodibenzo-p-dioxin (TCDD) at Seveso, Italy. Ann. N. Y. Acad Sci. 1979, 320, 311–320. [Google Scholar] [CrossRef]
- Tamburro, C.H. Chronic liver injury in phenoxy herbicide-exposed Vietnam veterans. Environ. Res. 1992, 59, 175–188. [Google Scholar] [CrossRef]
- O’Toole, B.I.; Marshall, R.P.; Grayson, D.A.; Schureck, R.J.; Dobson, M.; Ffrench, M.; Pulvertaft, B.; Meldrum, L.; Bolton, J.; Vennard, J. The Australian Vietnam Veterans Health Study: II. self-reported health of veterans compared with the Australian population. Int. J. Epidemiol. 1996, 25, 319–330. [Google Scholar] [CrossRef] [Green Version]
- Kang, H.K.; Dalager, N.A.; Needham, L.L.; Patterson, D.G.; Lees, P.S., Jr.; Yates, K.; Matanoski, G.M. Health status of Army Chemical Corps Vietnam veterans who sprayed defoliant in Vietnam. Am. J. Ind. Med. 2006, 49, 875–884. [Google Scholar] [CrossRef] [PubMed]
- Yi, S.W.; Ryu, S.Y.; Ohrr, H.; Hong, J.S. Agent Orange exposure and risk of death in Korean Vietnam veterans: Korean Veterans Health Study. Int. J. Epidemiol. 2014, 43, 1825–1834. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Serdar, B.; LeBlanc, W.G.; Norris, J.M.; Dickinson, L.M. Potential effects of polychlorinated biphenyls (PCBs) and selected organochlorine pesticides (OCPs) on immune cells and blood biochemistry measures: A cross-sectional assessment of the NHANES 2003-2004 data. Environ. Health 2014, 13, 114. [Google Scholar] [CrossRef] [Green Version]
- Czepiel, J.; Biesiada, G.; Gajda, M.; Szczepański, W.; Szypuła, K.; Dabrowski, Z.; Mach, T. The effect of TCDD dioxin on the rat liver in biochemical and histological assessment. Folia Biol. 2010, 58, 85–90. [Google Scholar] [CrossRef] [PubMed]
- Fowler, B.A.; Lucier, G.W.; Brown, H.W.; McDaniel, O.S. Ultrastructural changes in rat liver cells following a single oral dose of TCDD. Environ. Health Perspect. 1973, 5, 141–148. [Google Scholar] [CrossRef] [PubMed]
- Schecter, A.; Tiernan, T.; Schaffner, F.; Taylor, M.; Gitlitz, G.; VanNess, G.F.; Garrett, J.H.; Wagel, D.J. Patient fat biopsies for chemical analysis and liver biopsies for ultrastructural characterization after exposure to polychlorinated dioxins, furans and PCBs. Environ. Health Perspect. 1985, 60, 241–254. [Google Scholar] [CrossRef]
- Dwernychuk, L.W. Dioxin hot spots in Vietnam. Chemosphere 2005, 60, 998–999. [Google Scholar] [CrossRef] [PubMed]
- Hatfield Consultants, Office of National Committee 33, 2009. Comprehensive Assessment of Dioxin Contamination in Da Nang Airport, Viet Nam: Environmental Levels, Human Exposure and Options for Mitigating Impacts. (North Vancouver, BC, CANADA V7P0A3). Available online: http://www.hatfieldgroup.com/services/contaminant-monitoring-agent-orange/hatfield-agent-orange-reports-and-presentations/ (accessed on 21 January 2022).
- Tai, P.T.; Nishijo, M.; Kido, T.; Nakagawa, H.; Maruzeni, S.; Naganuma, R.; Anh, N.T.; Morikawa, Y.; Luong, H.V.; Anh, T.H.; et al. Dioxin concentrations in breast milk of Vietnamese nursing mothers: A survey four decades after the herbicide spraying. Environ. Sci. Technol. 2011, 45, 6625–6632. [Google Scholar] [CrossRef]
- Ministry of Health, Vietnam. Decision Number 5448/ 5448/QĐ-BYT on the Guidance for Diagnosis, Treatment of Hepatitis B Disease (in Vietnamese: Quyết định số 5448/QĐ-BYT: Về việc ban hành hướng dẫn chẩn đoán, điều trị bệnh viêm gan vi rút B); Ministry of Health, Vietnam: Hanoi, Vietnam, 2014; Available online: http://kcb.vn/thu-vien-tai-lieu/huong-dan-chan-doan-dieu-tri-benh-viem-gan-vi-rut-b.html/ (accessed on 28 March 2022).
- Olaf, P. PCDD/PCDF: Human background data for Germany, a 10-year experience. Environ Health Perspect. 1998, 106, 723–731. [Google Scholar]
- Jules, L.D. Chronic Hepatitis. In Harrison’s Principles of Internal Medicine, 19th ed.; McGraw Hill Education Medical: New York, NY, USA, 2015. [Google Scholar]
- Maria, G.; Alessandra, M.; Gavino, F. Chronic viral hepatitis: The histology report. Dig. Liver Dis. 2011, 43, S331–S343. [Google Scholar]
- Van den Berg, M.; Birnbaum, L.S.; Denison, M.; De Vito, M.; Farland, W.; Feeley, M.; Fiedler, H.; Hakansson, H.; Hanberg, A.; Haws, L.; et al. The 2005 World Health Organization reevaluation of human and mammalian toxic equivalency factors for dioxins and dioxin-like compounds. Toxicol. Sci. 2006, 93, 223–241. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Poynard, T.; Ratziu, V.; Benmanov, Y.; Di Martino, V.; Bedossa, P.; Opolon, P. Fibrosis in Patients with Hepatitis C: Detection and Significance: Detection and Significance. Semin. Liver Dis. 2000, 20, 56–68. [Google Scholar] [CrossRef] [PubMed]
- Van Luong, H.; Tai, P.T.; Nishijo, M.; Trung, D.M.; Thao, P.N.; Van Son, P.; Van Long, N.; Linh, N.T.; Nishijo, H. Association of dioxin exposure and reproductive hormone levels in men living near the Bien Hoa airbase, Vietnam. Sci. Total Environ. 2018, 628–629, 484–489. [Google Scholar] [CrossRef] [PubMed]
- Triebig, G.; Werle, E.; Päpke, O.; Heim, G.; Broding, C.; Ludwig, H. Effects of dioxins and furans on liver enzymes, lipid parameters, and thyroid hormones in former thermal metal recycling workers. Environ. Health Perspect. 1998, 106 (Suppl. S2), 697–700. [Google Scholar] [PubMed]
- Calvert, G.M.; Hornung, R.W.; Sweeney, M.H.; Fingerhut, M.A.; Halperin, W.E. Hepatic and gastrointestinal effects in an occupational cohort exposed to 2,3,7,8-tetrachlorodibenzo-para-dioxin. JAMA 1992, 267, 2209–2214. [Google Scholar] [CrossRef] [PubMed]
- Ott, M.G.; Zober, A.; Germann, C. Laboratory results for selected target organs in 138 individuals occupationally exposed to TCDD. Chemosphere 1994, 29, 2423–2437. [Google Scholar] [CrossRef]
- Greig, J.B.; Jones, G.; Butler, W.H.; Barnes, J.M. Toxic effects of 2,3,7,8-tetrachlorodibenzo-p-dioxin. Food Cosmet. Toxicol. 1973, 11, 585–595. [Google Scholar] [CrossRef]
- Lu, H.; Cui, W.; Klaassen, C.D. Nrf2 protects against 2,3,7,8-tetrachlorodibenzo-p-dioxin (TCDD)-induced oxidative injury and steatohepatitis. Toxicol. Appl. Pharmacol. 2011, 256, 122–135. [Google Scholar] [CrossRef] [Green Version]
- Maronpot, R.R.; Foley, J.F.; Takahashi, K.; Goldsworthy, T.; Clark, G.; Tritscher, A.; Portier, C.; Lucier, G. Dose response for TCDD promotion of hepatocarcinogenesis in rats initiated with DEN: Histologic, biochemical, and cell proliferation endpoints. Environ. Health Perspect. 1993, 101, 634–642. [Google Scholar] [CrossRef]
- Wolf, J.C.; Wheeler, J.R. A critical review of histopathological findings associated with endocrine and non-endocrine hepatic toxicity in fish models. Aquat Toxicol. 2018, 197, 60–78. [Google Scholar] [CrossRef]
- Dobrzyński, M.; Madej, J.P.; Leśków, A.; Tarnowska, M.; Majda, J.; Szopa, M.; Gamian, A.; Kuropka, P. The Improvement of the Adaptation Process of Tocopherol and Acetylsalicylic Acid in Offspring of Mothers Exposed to TCDD. Animals 2021, 11, 3430. [Google Scholar] [CrossRef]
- Ministry of Health, Vietnam. The Decision Number 09/2008/QĐ-BYT: Promulgating the List of Diseases, Deformities, Deformities, RELATED TO EXPosure to Toxic Chemicals/Dioxins (in Vietnamsese Quyết định số 09/2008/QĐ-BYT: Ban hành Danh mục bệnh, tật, dị dạng, dị tật có liên quan đến phơi nhiễm với chất độc hóa học/dioxin); Ministry of Health, Vietnam: Hanoi, Vietnam, 2008. Available online: http://vbpl.yte.gov.vn/van-ban-phap-luat/quyet-dinh-092008qd-byt.1.1855.html/ (accessed on 28 March 2022).
- Fernandez-Salguero, P.M.; Hilbert, D.M.; Rudikoff, S.; Ward, J.M.; Gonzalez, F.J. Arylhydrocarbon receptor-deficient mice are resistant to 2,3,7,8-tetrachlorodibenzo-pdioxin-induced toxicity. Toxicol. Appl. Pharmacol. 1996, 140, 173–179. [Google Scholar] [CrossRef]
- Mead, M.N. Cancer and TCDD: The mitochondrial connection. Environ. Health Perspect. 2008, 116, A112. [Google Scholar]
- Biswasm, G.; Srinivasan, S.; Anandatheerthavarada, H.K.; Avadhani, N.G. Dioxin-mediated tumor progression through activation of mitochondria-to-nucleus stress signaling. Proc. Natl. Acad. Sci. USA 2008, 105, 186–191. [Google Scholar] [CrossRef] [Green Version]
- Modica-Napolitano, J.S.; Singh, K.K. Mitochondrial dysfunction in cancer. Mitochondrion 2004, 4, 755–762. [Google Scholar] [CrossRef]


{kind=link}
| Characteristic | Unit | Mean (SD), N [%] | |
|---|---|---|---|
| Subjects | |||
| Age | year | 46.3 (12.1) | |
| Ratio of Male | % male | 16 [48.5%] | |
| Smoking Status | % smoker | 16 [48.5%] | |
| Alcohol Consumption | % drinking alcohol | 0 [0.0%] | |
| Length stayed in dioxin contaminated areas | Year | 26.0 (10.6) | |
| BMI | 21.7 (2.1) | ||
| METAVIR Score | |||
| F0 | % | 9 [17.3%] | |
| F1 | % | 14 [42.4%] | |
| F2 | % | 10 [30.3%] | |
| Dioxin Concentration in Blood | |||
| TCDD | pg/g lipid | 15.7 (3.7) * | |
| TEQ-PCDD/Fs | pg-TEQ/g lipid | 42.5 (2.5) * | |
| TCDD | TEQ-PCDD/FS | ||||||
|---|---|---|---|---|---|---|---|
| Markers | N | β | 95% CI (Lower, Upper) | p | β | 95% CI (Lower, Upper) | p |
| Aspartate Aminotransferase (AST) | 33 | 0.414 | (0.071, 0.758) | 0.020 | 0.393 | (0.046, 0.741) | 0.028 |
| Alanine Aminotransferase (ALT) | 33 | 0.359 | (0.009, 0.709) | 0.045 | 0.349 | (−0.003, 0.702) | 0.052 |
| Gamma-Glutamyl Transpeptidase (GGT) | 33 | 0.340 | (−0.020, 0.699) | 0.063 | 0.298 | (−0.068, 0.664) | 0.107 |
| Total Bilirubin | 33 | 0.389 | (0.030, 0.748) | 0.035 | 0.283 | (−0.091, 0.656) | 0.133 |
| Glucose | 33 | −0.05 | (−0.417, 0.318) | 0.79 | −0.14 | (−0.502, 0.229) | 0.45 |
| Urea | 33 | 0.031 | (−0.318, 0.381) | 0.855 | −0.013 | (−0.364, 0.337) | 0.938 |
| Creatinin | 33 | −0.011 | (−0.284, 0.262) | 0.933 | 0.062 | (−0.211, 0.334) | 0.648 |
| Protein | 33 | 0.421 | (0.104, 0.738) | 0.011 | 0.351 | (0.021, 0.680) | 0.038 |
| Cholesterone | 33 | 0.029 | (−0.334, 0.392) | 0.871 | 0.006 | (−0.358, 0.370) | 0.974 |
| Triglyceride | 33 | 0.043 | (−0.334, 0.420) | 0.816 | 0.104 | (−0.272, 0.480) | 0.576 |
| Red Blood Cells | 33 | 0.137 | (−0.200, 0.474) | 0.412 | 0.078 | (−0.263, 0.418) | 0.644 |
| Hemoglobin | 33 | 0.003 | (−0.288, 0.294) | 0.985 | −0.024 | (−0.316, 0.267) | 0.866 |
| Leukocytes | 33 | −0.031 | (−0.420, 0.357) | 0.870 | −0.225 | (−0.605, 0.155) | 0.236 |
| Neutrocytes | 33 | −0.201 | (−0.582, 0.181) | 0.291 | −0.240 | (−0.619, 0.139) | 0.205 |
| Lymphocytes | 33 | 0.234 | (−0.146, 0.614) | 0.218 | 0.299 | (−0.075, 0.673) | 0.113 |
| Platelets | 33 | −0.172 | (−0.549, 0.206) | 0.360 | −0.127 | (−0.508, 0.254) | 0.500 |
| Histopathological Damage | Yes N (%) | No N (%) |
|---|---|---|
| Granular Degeneration | 32 (97.0) | 1 (3.0) |
| Hydropic Degeneration | 33 (100) | 0 (0.0) |
| Lipoic Degeneration | 32 (97.0) | 1 (3.0) |
| Lipogranuloma | 0 (0.0) | 33 (100) |
| Lymphocytes and Polynuclear Leukocytes Surrounding the Liver Cells | 33 (100) | 0 (0.0) |
| Mallory Bodies | 0 (0.0) | 33 (100) |
| Pigmentation | 0 (0.0) | 33 (100) |
| Megamitochondria | 0 (0.0) | 33 (100) |
| Changes in Acidophil Hepatocyte | 4 (12.1) | 29 (87.9) |
| Venous Obstruction | 0 (0.0) | 33 (100) |
| OR | SE | 95% CI (Lower, Upper) | p | |
|---|---|---|---|---|
| TCDD | 5.9 | 0.7 | (1.6, 21.4) | 0.007 |
| TEQ-PCDDs/Fs | 3.9 | 0.6 | (1.2, 12.1) | 0.021 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pham, P.Q.; Nguyen, V.B.; Pham, T.T.; Duong, N.X.; Nguyen, H.T.; Ha, Q.V.; Nguyen, T.D.; Hoang, T.M.; Dinh, D.T.; Tran, Q.T.N.; et al. Histopathological Alterations in the Livers of Chronic Hepatitis Patients Exposed to Agent Orange/Dioxin in Vietnam. Toxics 2022, 10, 315. https://doi.org/10.3390/toxics10060315
Pham PQ, Nguyen VB, Pham TT, Duong NX, Nguyen HT, Ha QV, Nguyen TD, Hoang TM, Dinh DT, Tran QTN, et al. Histopathological Alterations in the Livers of Chronic Hepatitis Patients Exposed to Agent Orange/Dioxin in Vietnam. Toxics. 2022; 10(6):315. https://doi.org/10.3390/toxics10060315
Chicago/Turabian StylePham, Phu Quang, Vuong Ba Nguyen, Tai The Pham, Nhuong Xuan Duong, Ha Trong Nguyen, Quang Van Ha, Thuan Duc Nguyen, Tuan Minh Hoang, Dong Tien Dinh, Quynh Thi Nhu Tran, and et al. 2022. "Histopathological Alterations in the Livers of Chronic Hepatitis Patients Exposed to Agent Orange/Dioxin in Vietnam" Toxics 10, no. 6: 315. https://doi.org/10.3390/toxics10060315